WHAT IS THORACIC OUTLET SYNDROME (TOS)?
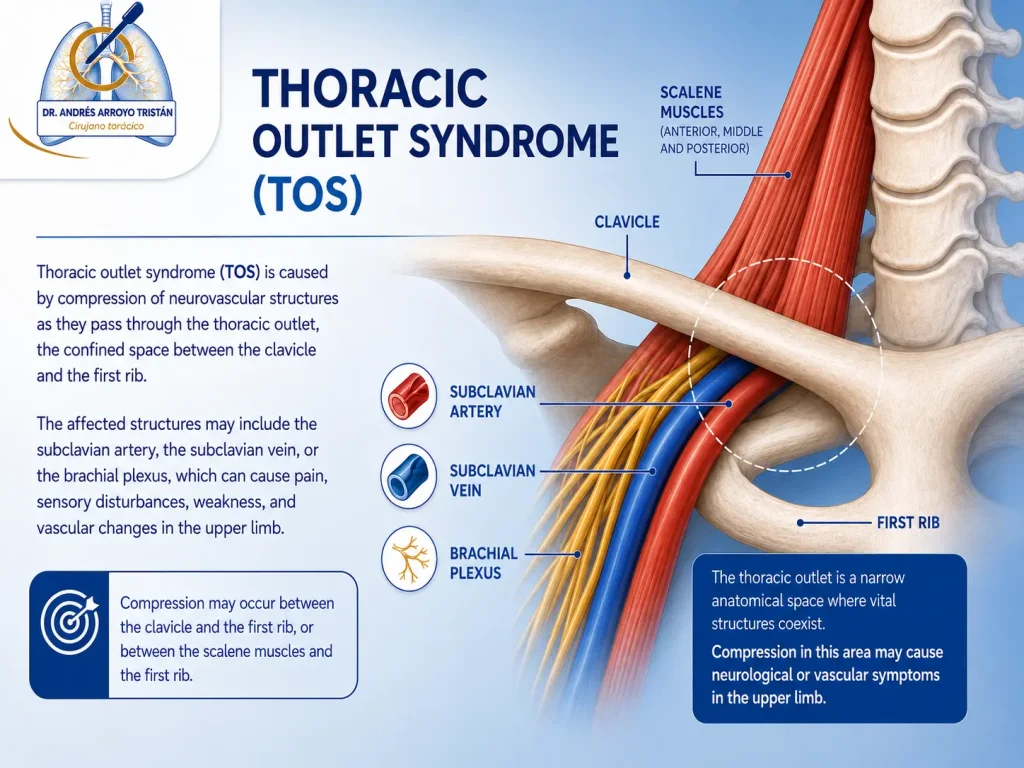
Thoracic Outlet Syndrome (TOS) includes a group of disorders caused by the compression of neurovascular structures as they pass from the neck to the upper limb through the thoracic outlet. Depending on the affected structure, three main clinical forms are distinguished: neurological, venous and arterial.

The most common form is neurological TOS, caused by compression of the brachial plexus. It usually manifests with neck and shoulder pain, tingling, a feeling of weakness, loss of strength and sensory disturbances in the arm or hand.
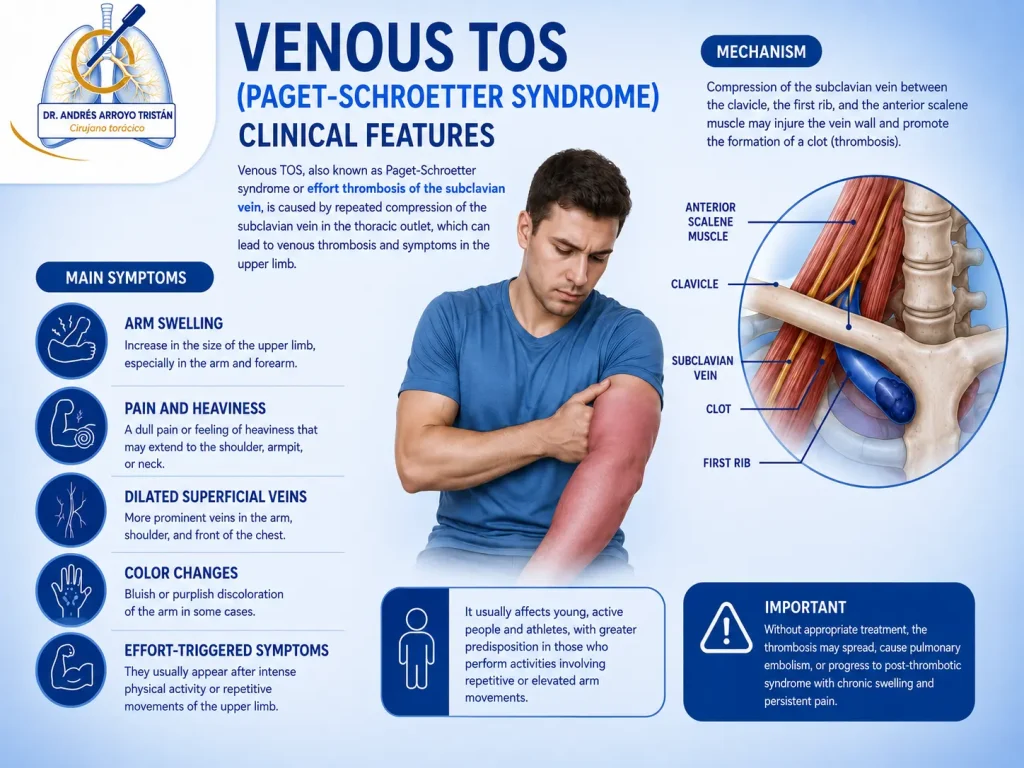
Venous TOS, also known as Paget-Schroetter syndrome or effort thrombosis of the subclavian vein, occurs due to repeated compression of the vein between the clavicle and the first rib. It usually affects young and active patients and may be triggered by intense exercise or repetitive movements of the upper limb. Clinically, it causes arm swelling, heaviness, pain, changes in coloration and the appearance of superficial venous circulation.
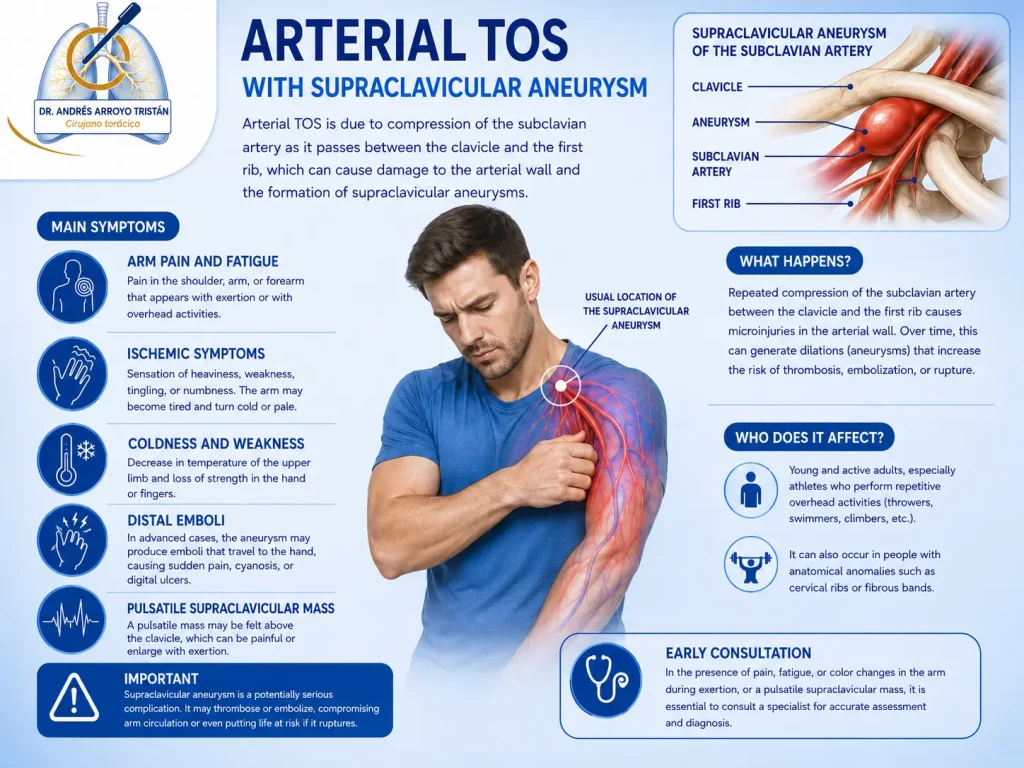
Finally, arterial TOS is the least common variant, but potentially the most serious. It is caused by compression of the subclavian artery, often associated with bone abnormalities such as cervical ribs. It may cause pain, coldness, loss of strength, arm claudication or episodes of distal embolization.
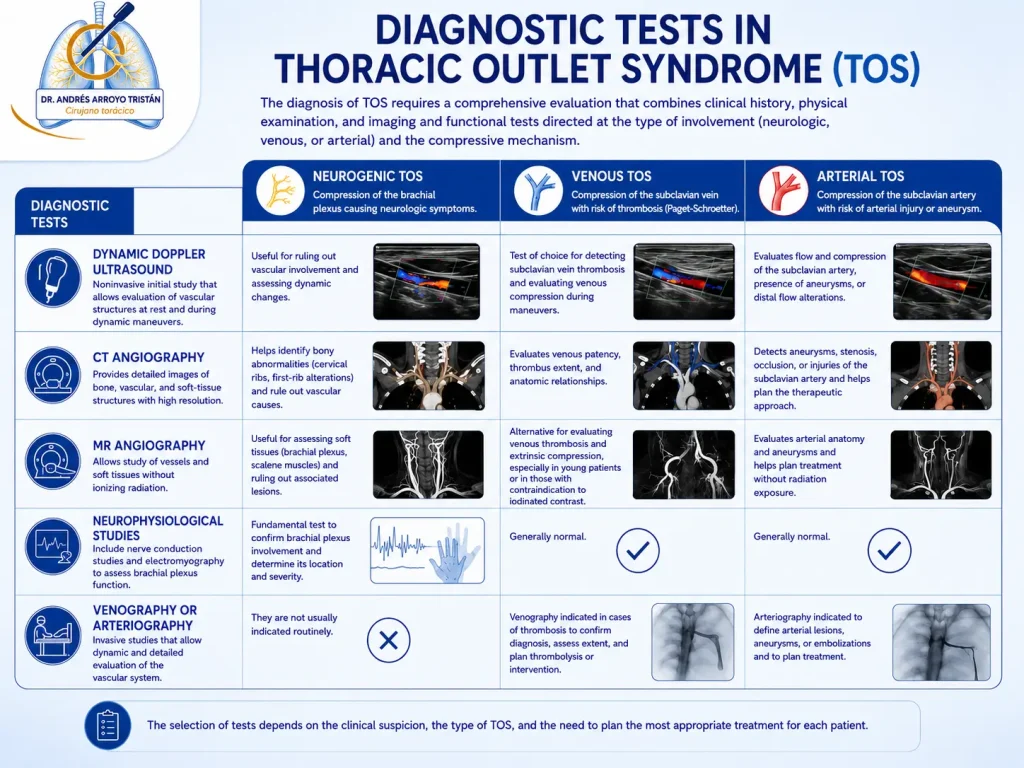
Diagnosis requires a detailed clinical assessment, specific physical examination and imaging studies aimed at identifying the compressive mechanism. The most commonly used tests include dynamic Doppler ultrasound, CT angiography, MR angiography, neurophysiological studies and, in selected cases, venography or arteriography to characterize vascular involvement and plan treatment.
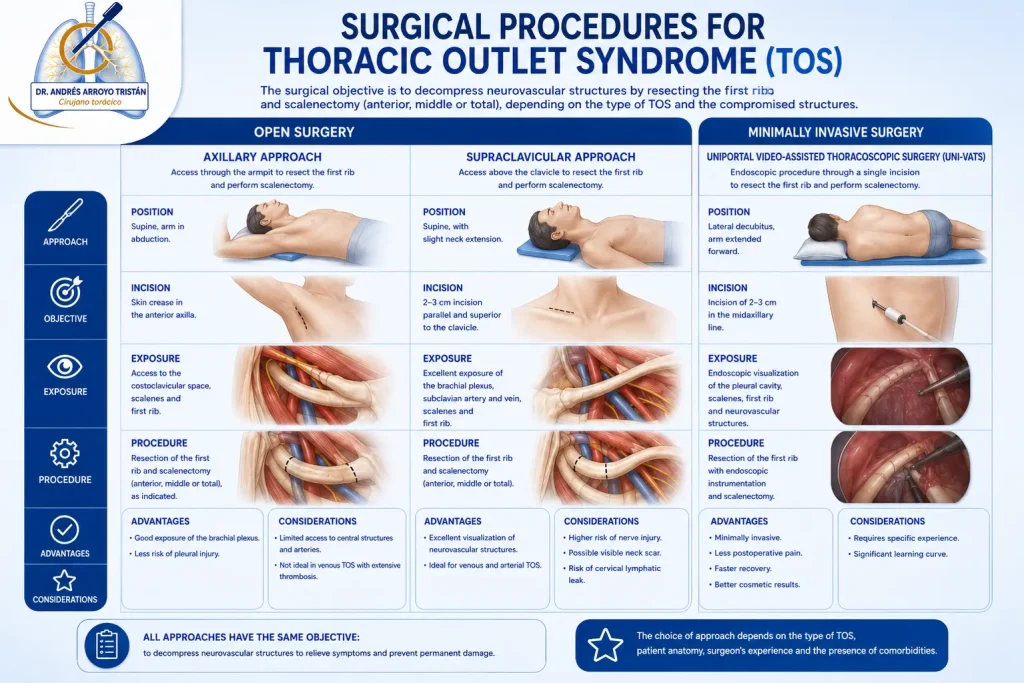
Treatment depends on the subtype and the severity of the symptoms. In selected patients, especially in Paget-Schroetter syndrome and in certain refractory arterial or neurological forms, surgical treatment represents a definitive option. The aim is to decompress the thoracic outlet, usually through resection of the first rib, combined when necessary with muscle release, scalenectomy and complementary vascular procedures.
Historically, this surgery was performed through open approaches, mainly axillary and supraclavicular, effective techniques but with limitations in anatomical exposure and postoperative recovery.
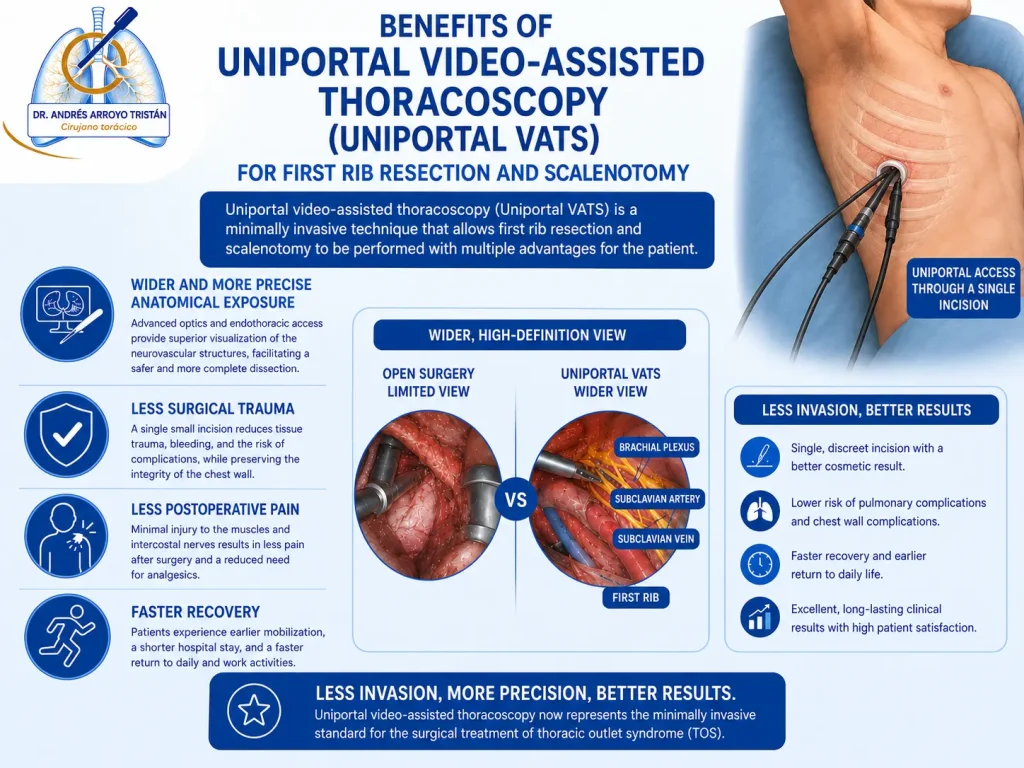
In recent years, the development of minimally invasive video-assisted thoracoscopic surgery (VATS) has made it possible to perform first rib resection with an expanded view of the neurovascular structures, less surgical trauma and faster recovery in appropriately selected patients.
Current management of TOS requires a multidisciplinary assessment and an individualized selection of treatment to restore upper limb function, relieve symptoms and prevent long-term vascular sequelae.
TOS POR COSTILLA CERVICAL
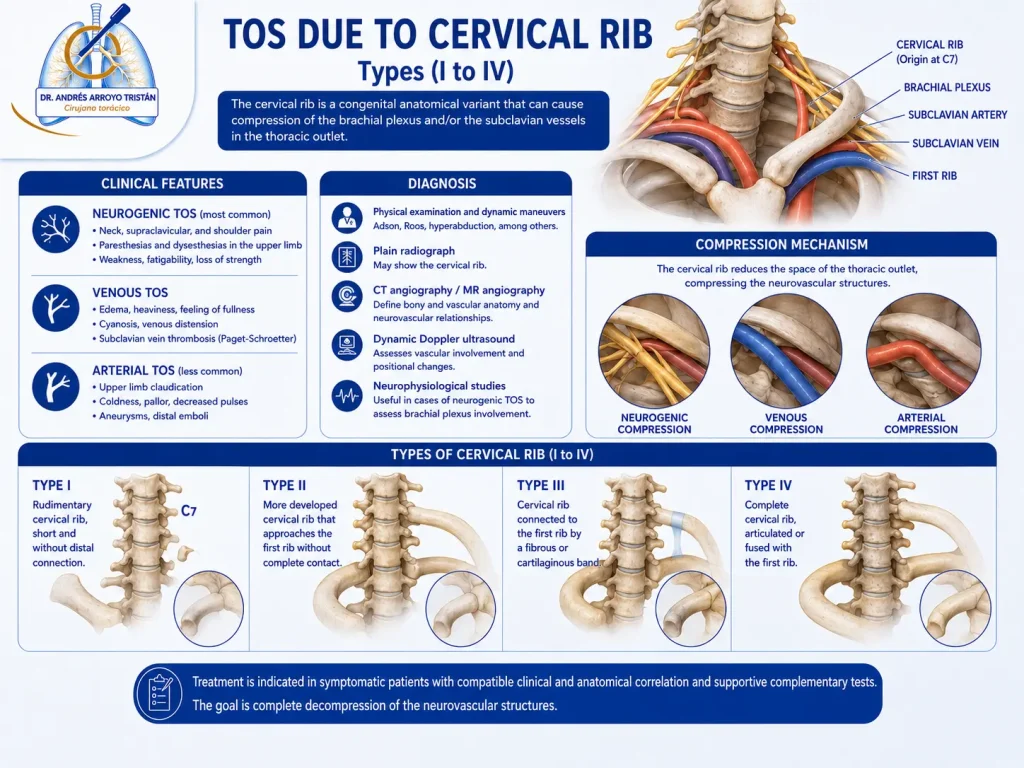
Thoracic Outlet Syndrome (TOS) due to cervical rib is an anatomical form of neurovascular compression caused by the presence of a cervical rib, a congenital variant that usually arises from the seventh cervical vertebra and reduces the available space for the passage of the brachial plexus and the subclavian vessels. Although many cervical ribs remain asymptomatic throughout life, in certain patients they may generate progressive compression and cause neurological, venous or arterial symptoms. Classically, four anatomical types (I–IV) are described: type I, a short rudimentary rib with no distal connection; type II, a more developed rib that approaches the first rib without complete contact; type III, partial union through a fibrous band; and type IV, a complete cervical rib articulated or fused with the first rib.
Clinical presentation depends on the compromised structure, with neurological TOS usually predominating, causing cervical and supraclavicular pain, radiation to the upper limb, paresthesias, loss of strength and fatigability. In cases of vascular involvement, edema, color changes, coldness, arm claudication or distal embolic phenomena may appear.
Diagnosis requires a combination of targeted clinical examination, dynamic maneuvers and imaging tests aimed at defining both the anatomy and the compressive mechanism. Plain radiography usually allows identification of the cervical rib, while CT angiography and MR angiography provide detailed anatomical information about its relationship with the subclavian artery and vein and the brachial plexus; dynamic Doppler ultrasound helps assess vascular impact, and neurophysiological studies may complement the evaluation in selected neurological forms.

In patients with persistent symptoms or significant neurovascular involvement, surgical treatment aims to achieve complete decompression of the thoracic outlet. An advanced strategy consists of combined surgery through first rib resection using uniportal video-assisted thoracoscopic surgery (Uniportal VATS), which provides an expanded endothoracic view and precise resection of the lower costal component, associated with section or resection of the cervical rib through a supraclavicular approach, allowing release of the brachial plexus and vascular structures from the cervical compartment.
This approach combines the advantages of minimally invasive surgery with direct exposure of the cervical rib and aims to achieve complete anatomical decompression with less surgical trauma and faster recovery.