WHAT IS PNEUMOTHORAX?
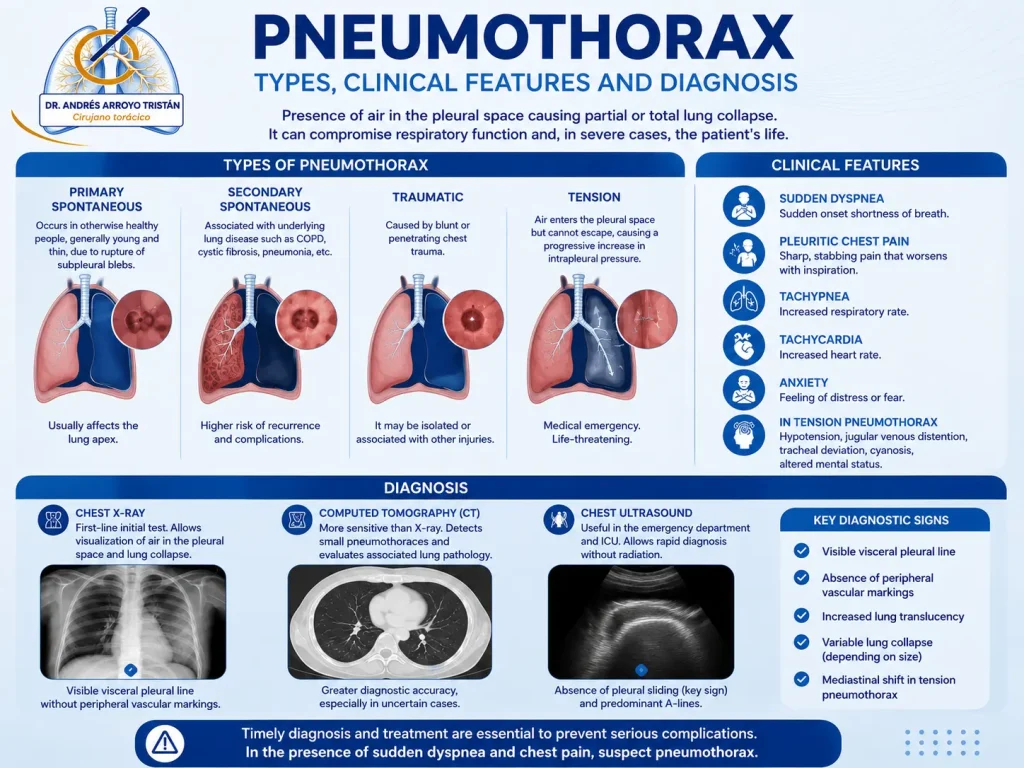
Pneumothorax consists of the presence of air within the pleural cavity, causing a partial or complete separation between the lung and the chest wall and resulting in lung collapse of varying severity. Depending on its cause, it can be classified as primary spontaneous pneumothorax, which usually appears in young patients with no known lung disease and is often related to the rupture of subpleural bullae or blebs; secondary spontaneous pneumothorax, associated with previous lung diseases such as COPD, emphysema or interstitial diseases; traumatic pneumothorax, secondary to chest trauma; and iatrogenic pneumothorax, related to medical procedures. The most severe form is tension pneumothorax, a potentially urgent situation due to respiratory and haemodynamic compromise.
The clinical presentation is usually characterised by the sudden onset of pleuritic chest pain, shortness of breath, a sensation of chest tightness and, occasionally, a dry cough. The intensity of the symptoms depends on the size of the pneumothorax, the speed of onset and the patient’s baseline lung function. Diagnosis is based on the medical history and physical examination, complemented by chest X-ray, which remains the most commonly used initial test. In selected cases, especially when it is necessary to assess underlying lung disease, identify bullae or plan surgical treatment, a computed tomography (CT) scan of the chest may be performed.
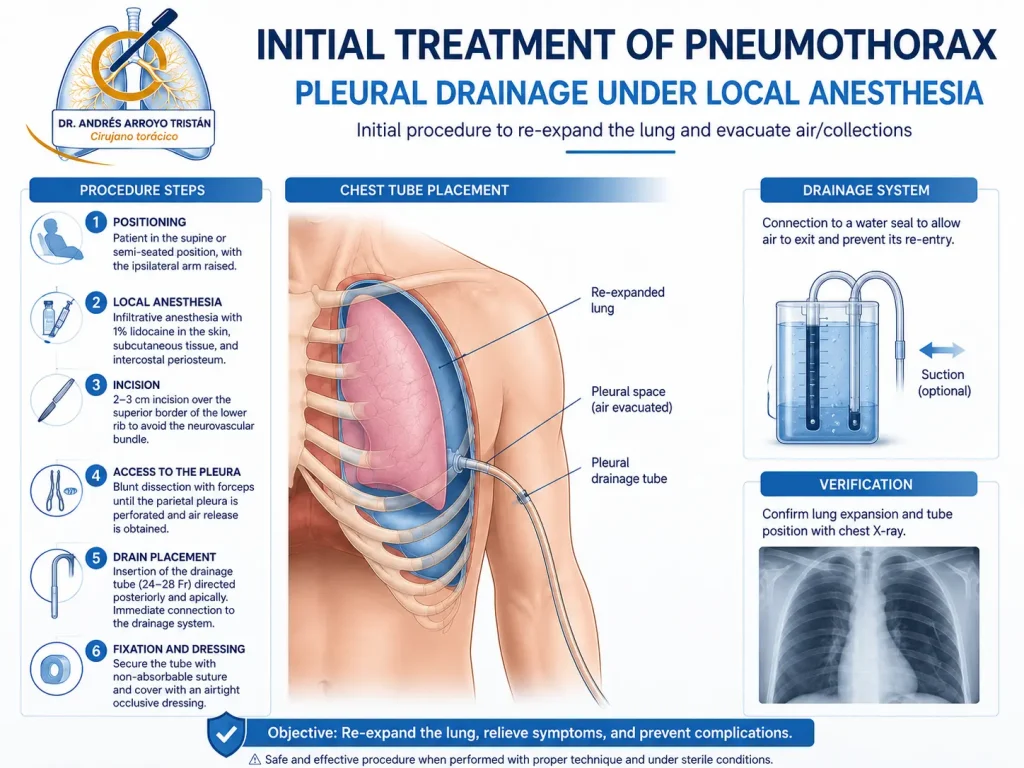
Treatment depends on the size of the pneumothorax, the symptoms and the risk of recurrence. Some small forms can be managed with observation and oxygen therapy, while others require air evacuation through pleural drainage.
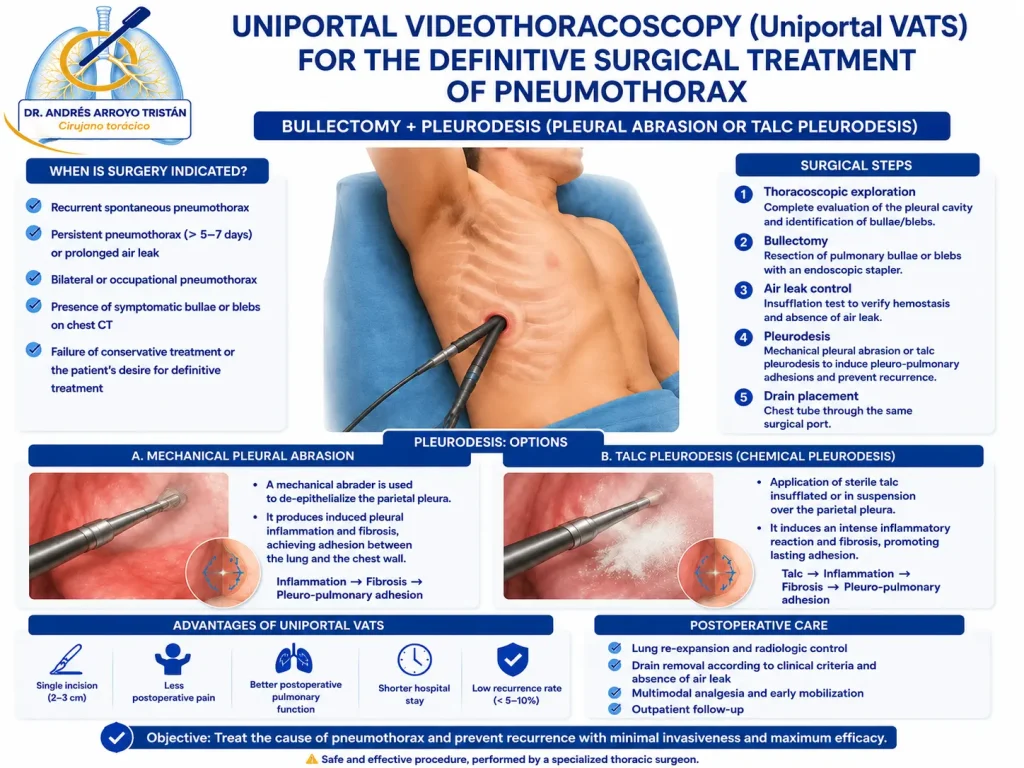
In patients with recurrent episodes, persistent air leak, bilateral pneumothorax, high-risk professions or the presence of apical bullae, surgical treatment represents a definitive option. The most commonly used current strategy consists of minimally invasive surgery through uniportal videothoracoscopy (Uniportal VATS). Uniportal VATS surgery allows complete treatment through a single small incision, usually lateral and intercostal. The procedure includes the removal of pulmonary bullae or blebs (bullectomy) responsible for the air leak, generally using mechanical sutures, associated with a technique to promote adhesion between the lung and the chest wall and reduce the risk of recurrence.
For this purpose, mechanical pleural abrasion or chemical pleurodesis using pleural talc poudrage may be performed, selecting the most appropriate strategy for each patient.
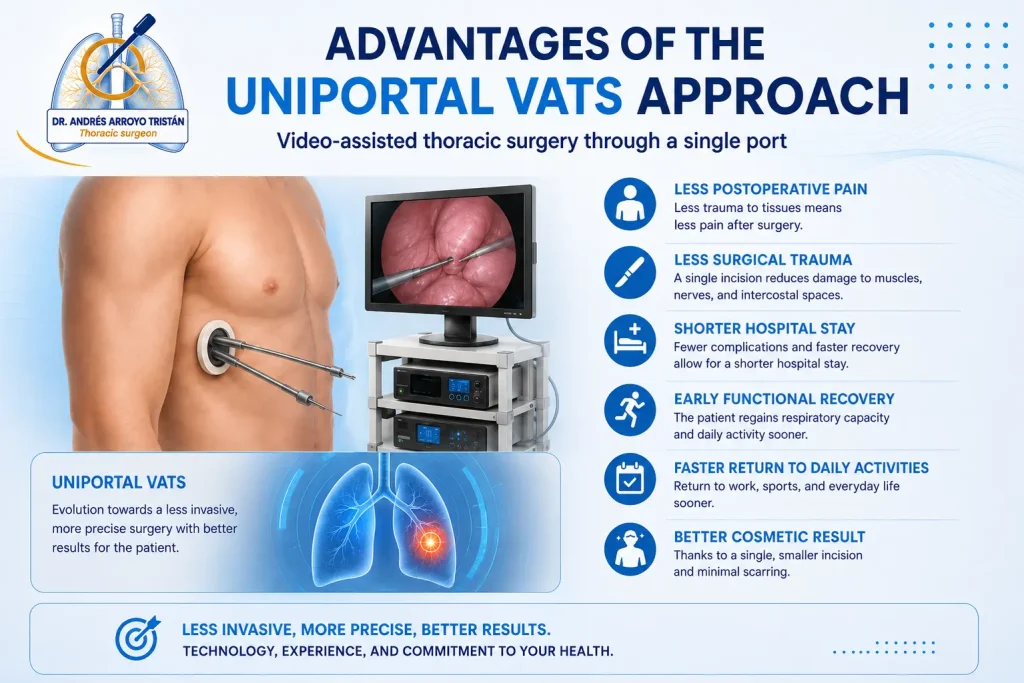
Among the main benefits of uniportal videothoracoscopy are reduced surgical trauma, an enlarged and precise view of the pleural cavity, less postoperative pain, better cosmetic results, shorter hospital stay and faster recovery with an earlier return to normal activity. In addition, it maintains excellent results in controlling air leaks and reducing the risk of pneumothorax recurrence, establishing itself as one of the reference techniques in the modern surgical treatment of this disease.